
New-onset seizures as an early warning for brain tumors
A first seizure is scary and disorienting. Convulsions, losing control of the body or limbs, talking incoherently, intense and unusual feelings such as deja vu, or having the mind go blank right in the middle of a conversation are all possible symptoms of a new-onset seizure.
It usually goes away as fast as it came, but that time when the body and brain aren’t responsive feels like a lifetime. Seizures without a known cause are signs of trouble, but they’re also an opportunity for diagnosis.
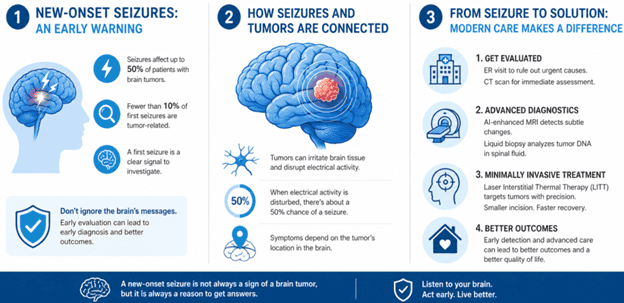
According to the American Cancer Society, seizures can be an early warning of a brain tumor. They affect up to 50% of patients with brain tumors, but fewer than 10% of first seizures are tumor related. A new-onset seizure is a clear invitation for further investigation.
Neurosurgery One, a specialized neurological center, examines the connection between new-onset seizures and brain tumors.
New-onset seizures are a diagnostic opportunity
Seizures are not as uncommon as they may seem. Research says that 8% to 10% of the world population will experience one during their lifetime. Plus, in most cases, they don’t always look like what people see in movies.
There are billions of nerve cells in the human brain working together to keep the body moving, thinking and feeling. But to function optimally, these cells need a stable environment. Even the smallest change can throw this fine-tuned biological machine out of whack.
A first seizure, without any apparent cause, especially as an adult, is a clear sign that something isn’t working right inside the brain. Even if there is an apparent cause, like epilepsy, it could still be an early sign of a brain tumor, especially if an epilepsy diagnosis came during adulthood.
The brain tumor-seizure link
Tumors, especially slow-moving ones like low-grade gliomas, gangliogliomas and dysembryoplastic neuroepithelial tumors, irritate the brain tissue and interfere with the brain’s electrical activity.
Seizures occur when the brain has a sudden, uncontrollable surge of electrical activity. Depending on where the tumor is located in the brain, the symptoms are different. For instance, if the tumor is close to the optic nerve, it may impact vision. On the other hand, some patients report strong odors or numbness in their limbs.
According to the Handbook of Clinical Neurology, glioneuronal tumors are the most likely to cause seizures. However, not all present with seizures. Low-grade gliomas seem to be the most likely culprit, especially in patients under 50.
What to do after a first-time seizure
Few things are more frightening than a sudden loss of motor control. It’s not always a sign of brain cancer, but it is serious enough to start investigations immediately.
Start with an ER visit. The goal here is to rule out immediate life-threatening triggers like strokes, severe electrolyte imbalances, or active brain bleeds. A CT scan can quickly rule out large tumors or hemorrhages.
Once stable, it’s time to start looking for the reason behind the patient’s condition. By now, there should be a better understanding about the type of seizure and its possible causes. The gold standard is a high-resolution magnetic resonance imaging (MRI) of the brain and an electroencephalography.
Medical experts note that modern diagnostic tools have significantly reduced the invasive nature of brain mapping.
AI-Enhanced Volumetric MRI
Standard MRIs provide pictures of the brain that doctors use to figure out what caused the seizure. Radiologists use AI layers to detect subtle cortical thickening that standard imaging can miss, specifically in patients presenting with new-onset epilepsy.
The scanner captures the brain in thin slices, which the AI assembles into a detailed 3D model. Next, the AI compares the brain’s volume against a massive database of healthy scans and detects even the smallest anomalies.
CNS-Specific Liquid Biopsies
To confirm a seizure was tumor-provoked, doctors also run a CNS-specific liquid biopsy, a minimally invasive procedure that requires a lumbar puncture (spinal tap).
It’s the easiest way to analyze the genetic and molecular profiles of a brain or spinal cord condition without surgically removing tissue. Existing brain tumors, even microscopic ones, shed DNA fragments into the cerebrospinal fluid, and a biopsy will reveal their presence.
When used alongside imaging, CNS-specific liquid biopsies help confirm if a seizure was tumor-provoked.
Laser Interstitial Thermal Therapy (LITT)
Neurosurgeons can sometimes bypass the need for a traditional craniotomy. Instead, they use laser interstitial thermal therapy (LITT), which is a minimally invasive neurosurgical procedure that uses laser-generated heat in place of a scalpel.
For this procedure, the point of entry is a tiny hole in the skull, roughly the diameter of a pencil. Through this orifice, the neurosurgeon introduces a thin fiber-optic wire that is guided to the target using real-time MRI navigation.
Once in place, the laser delivers controlled thermal energy to cook and kill the targeted tissue from the inside out. Since the MRI monitors temperature in real time, the surrounding healthy brain tissue won’t be affected.
Because the incision is tiny, patients typically recover much faster than they would from traditional open-brain surgery, often going home the next day.
Don’t ignore your brain’s messages
A new-onset seizure is not always a sign of a brain tumor, and a tumor doesn’t always cause seizures. However, newly experienced symptoms, seizures, or a diagnosis of epilepsy as an adult means that it’s time to contact a physician.

