

As an interventional pain medicine physician specializing in back and neck pain, I often get asked what is the best painkiller for spinal stenosis. After all, spinal stenosis — often called by its most common symptom, sciatica — is a frequently experienced spinal condition that causes pain.
To understand the best painkiller, we need to look first at exactly what spinal stenosis is and how it causes pain. Stenosis comes from the Greek word stenos, which means narrow. In this case, it’s a narrowing of the spinal canal that puts pressure on a nerve and causes numbness, tingling, pain and sometimes weakness in the arms or legs. Those symptoms are known as radiculopathy, or sciatica when it’s pain running down the back of the legs.
Spinal stenosis can cause pain by inflammation or irritation of the nerve roots, so we use various medications targeting these pathways. It’
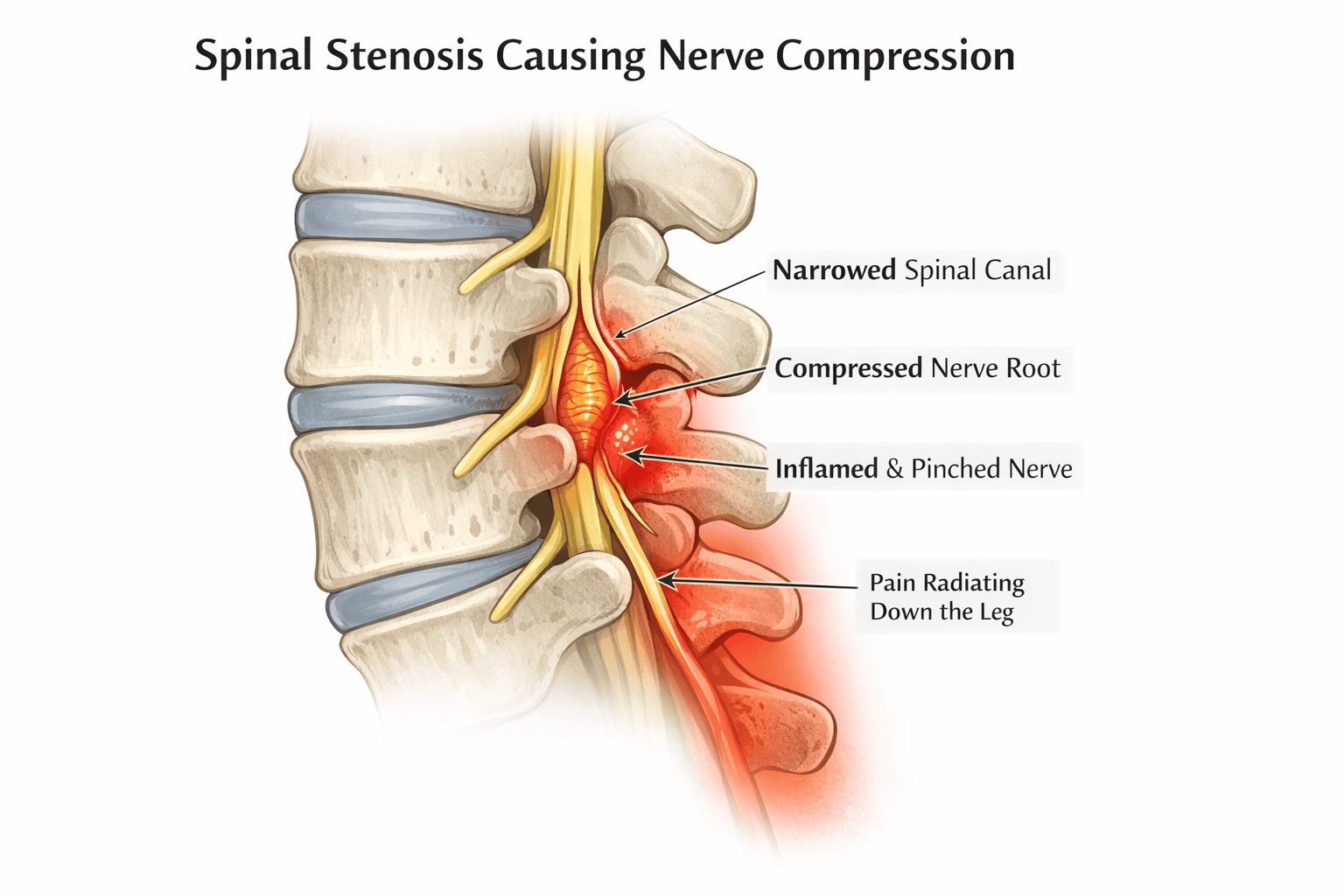
s important to note that these medications are short-term treatments meant to provide immediate pain relief and are best used as soon as possible when pain occurs. Pain medication is the closest thing we have to a band-aid when it comes to spine pain — it helps temporarily stop symptoms but doesn’t address the cause of the problem.
With that said, let’s look at the two best painkillers for spinal stenosis.
Steroids and Non-steroidal Anti-inflammatory Drugs (NSAIDs)
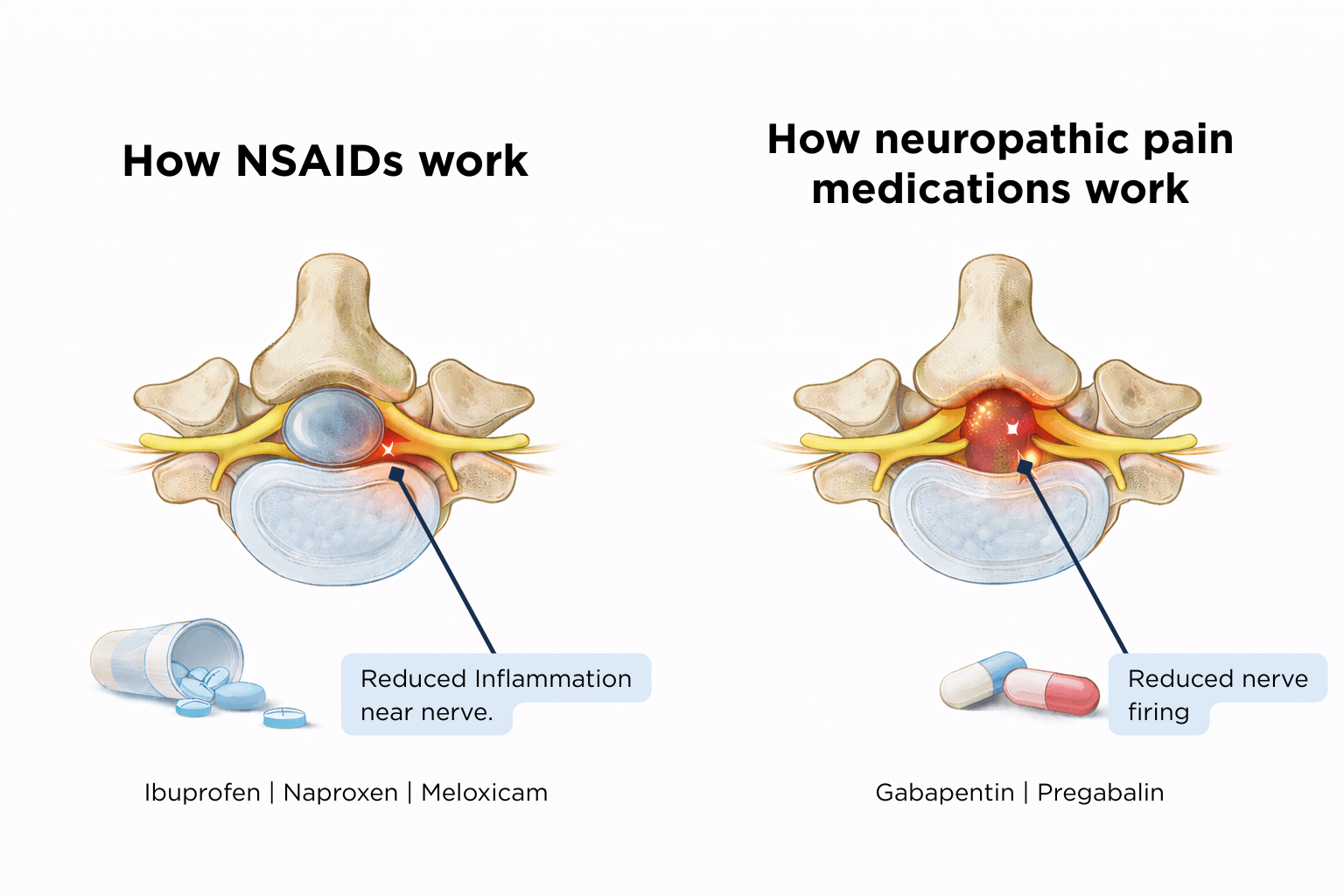
When a narrowed spinal canal puts pressure on a nerve, it sets off an inflammatory process that sensitizes nerve endings, lowers pain thresholds, increases swelling (which compresses the nerves even further) and increases pain and stiffness. Both steroids and NSAIDs can help reduce inflammation, bringing almost immediate pain relief.
Common over-the-counter NSAIDs include ibuprofen and naproxen. There are no over-the-counter steroids available to treat pain. Because NSAIDs are easily accessible, I recommend using these immediately with the onset of pain if you have no health issues that prevent use, such as allergies, kidney problems or are on blood thinners (talk to your doctor to make sure you can safely take NSAIDs).
Be sure to take the full dose as often as allowed for 1-2 weeks. I also recommend using ice, gentle exercise and stretching (don’t stay in bed). If you are able to tolerate it, physical therapy can be helpful during the acute pain response, but also for prevention of future episodes by strengthening the core and improving mobility.
If you have a sudden back or neck injury that stops you from going to work or engaging in daily living activities, you may benefit from prescription NSAIDs or oral steroids. (If you are in this situation and are not experiencing any red flag symptoms, call us to schedule an appointment in our Back & Neck Pain Clinic at 720-419-3080.)
Neuropathic Pain Medications
The second type of painkiller for spinal stenosis addresses irritation of the nerve roots causing neuropathic pain –- pain stemming from the nervous system and usually described as burning, shooting, tingling, or pins and needles. Gabapentin and pregabalin are the most commonly used drugs that target neuropathic pain. These medications work by reducing the release of neurotransmitters involved in pain signaling, reducing the number of pain signals that reach the brain. These medications take time to build up in the system, and generally are taken on a regular basis rather than only when pain strikes.
The Pros and Cons of Painkillers for Spinal Stenosis
The biggest benefit of these medications is that both classes of painkillers work well in controlling radiculopathy caused by spinal stenosis, particularly when taken at the first sign of pain. Acute pain responds far better to these drugs than chronic pain, which can become centralized over time and harder to treat.
Most people experience strong relief when NSAIDs are used consistently for a short period. Gabapentin and pregabalin have varied results: These medications tend to work better at higher doses, but many people may not be able to tolerate those doses due to side effects. Older adults are particularly sensitive, which makes their response even more variable.
The biggest downsides to these pain medications are side effects and the fact that they don’t work for long. Both classes of drugs come with potential side effects that must be considered.
NSAIDs should not be taken for longer than a few weeks to one month at the most. Side effects of long-term use include:
- Kidney problems
- Stomach irritation or ulcers
- Additional bleeding risk for people on blood thinners
- Increased risk of heart attack, stroke, hypertension
Gabapentin and pregabalin can cause a variety of side effects, including:
- Drowsiness or fatigue
- Dizziness
- Brain fog
Older adults tend to be more sensitive to these effects. They also require a gradual taper when starting or stopping. Stopping abruptly can lead to withdrawal symptoms like anxiety, insomnia or nausea.
Painkillers Don’t Fix the Underlying Problem
A common misconception is that pain medication cures spinal stenosis. It does not. Both NSAIDs and neuropathic medications can provide short-term symptom relief, but they do not correct the narrowing around the nerve root that is causing the pain.
For some individuals, short-term relief is all they need. Others may find their symptoms return as soon as they stop the medication. Understanding which group you fall into is key to knowing whether painkillers will be enough or whether you will eventually need a more targeted treatment.
When Medication Is Enough
Some people take NSAIDs for a brief flare and their pain settles. They can go weeks or months without another issue. Others take medication while their body naturally corrects the problem. For example, when stenosis is caused by a herniated disc, the body can break down and absorb the herniated disc material over time, reducing pressure on the nerve and improving symptoms. Medication simply helps them get through that early phase until the space around the nerve opens again.
When Medication Isn’t Enough
If stenosis is caused by degenerative changes like enlarged joints, thickened ligaments or long-standing disc degeneration, painkillers may reduce symptoms temporarily but will not resolve the root issue. These patients often need a longer-term treatment strategy such as:
- Epidural Steroid Injections: These injections place steroid medication right next to the irritated nerve root. They can be repeated every few months and often provide longer lasting relief than oral medication. Injections treat the inflammation more directly, with fewer systemic side effects.
- Spinal Cord Stimulation: This option is effective for people whose symptoms travel down the legs. It is often offered when injections or medications do not provide adequate relief. Because this technique can be tried out with a temporary device, patients can be sure it works before having a permanent implant. It also can be adjusted to fit the patient’s needs.
- Surgery: Surgery is appropriate when the stenosis is severe, symptoms are progressive or red flag symptoms appear, such as weakness in the arms or legs, or bowel or bladder changes. Surgery can be performed with minimally invasive procedures.
Final Thoughts
Finding the best painkiller for spinal stenosis depends on the cause of the narrowing, how early treatment begins and how your body responds to short-term medications. Painkillers can be extremely helpful for symptom relief but should be viewed as temporary tools rather than permanent solutions. For many patients, medications can serve as an important first step before the body heals or before a more targeted treatment is delivered.
